Sleep Is Part of Physical Therapy Recovery
Sleep is not downtime between one physical therapy session and the next. It is one of the times when your body repairs tissue, regulates pain, and stores the movement skills you are practicing.
For many veterans, good sleep is not simple. Pain, PTSD, traumatic brain injury (TBI), medications, and disrupted routines can make sleep light, broken, or unrefreshing. That does not mean you are failing. It means sleep deserves clinical attention inside your recovery plan.
Why sleep matters for recovery
During deep sleep, your body releases growth hormone, a signal that helps repair muscle, tendons, ligaments, and other tissues. The connection between deep sleep and tissue repair has been documented for decades. A study published in Physiological Reports (2021) found that one night of total sleep loss reduced muscle protein synthesis in young adults, though that finding should be treated as a warning sign, not a rule for every person.
Sleep also helps your brain keep what you practice. Rehabilitation is not only about strengthening a muscle. It is also about relearning balance, coordination, and control. A meta-analysis of 48 studies published in Neuroscience & Biobehavioral Reviews found that sleep improves motor memory consolidation. In plain language: what you practice during the day sticks better when you sleep.
Here is the recovery chain at a glance:
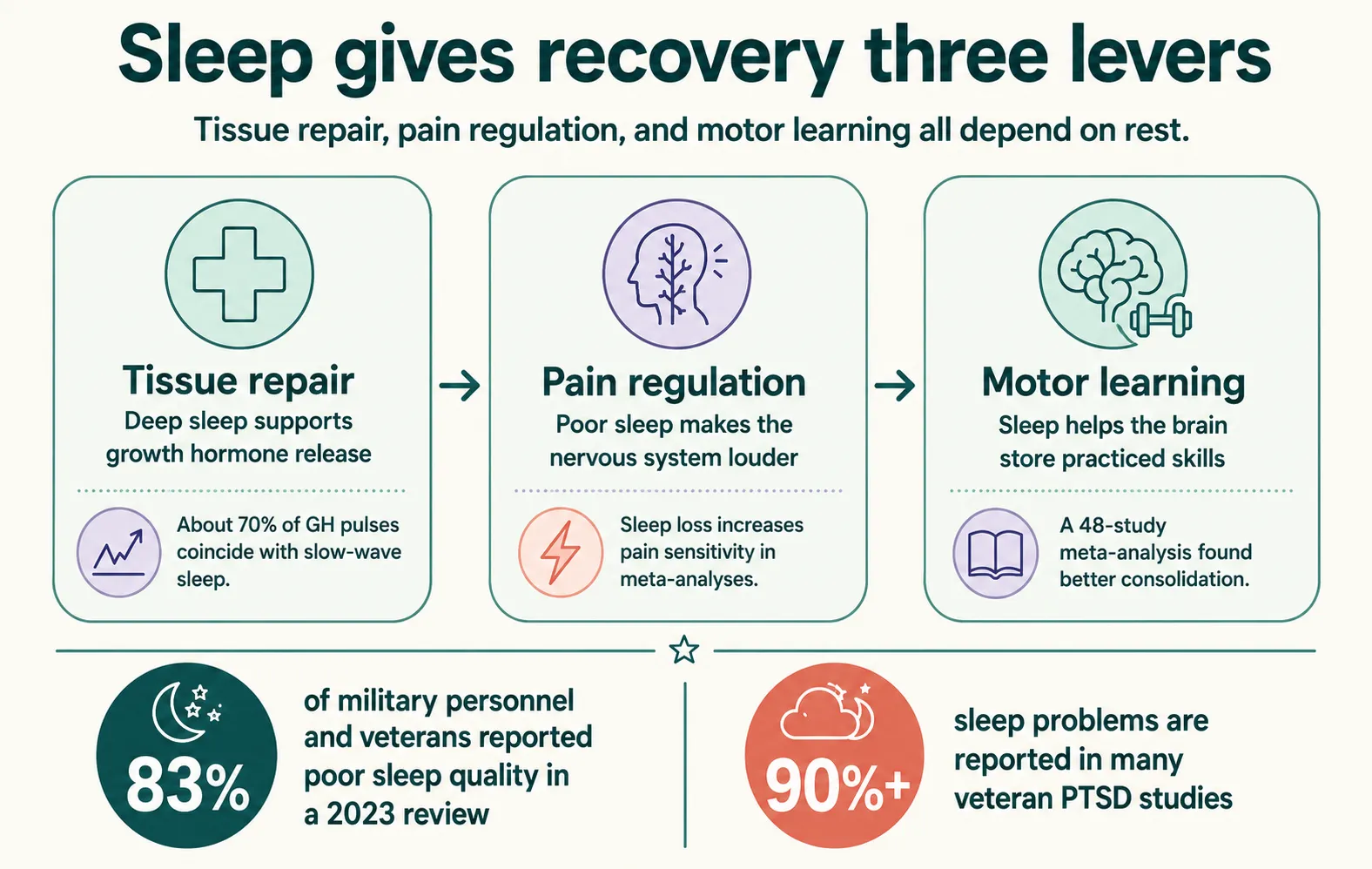
How poor sleep amplifies pain
Pain and sleep affect each other in both directions, but research shows sleep often carries more weight. A review published in The Journal of Pain (2013) found that sleep problems predicted next-day pain more strongly than pain predicted later sleep. A 2024 meta-analysis in Pain, including more than 116,000 participants, found that sleep problems increased the risk of chronic musculoskeletal pain.
When you sleep poorly, your nervous system becomes more sensitive. Your brain has less ability to turn down pain signals, and after several days of short sleep, your body may produce more inflammatory signals. This does not mean the pain is “in your head.” It means your nervous system is working with less recovery and more threat.
Why veterans experience this more often
Sleep problems are much more common in veterans than in the general population. A review of 59 studies published in Sleep Medicine Reviews (2023) found that nearly 83% of military personnel and veterans had poor sleep quality. Among veterans with PTSD, sleep problems are even more common; multiple studies report rates above 90%.
Sleep apnea also deserves attention. Loud snoring, pauses in breathing, waking up gasping, morning headaches, or daytime sleepiness can point to a problem that needs medical evaluation. Physical therapy can help screen for warning signs, but PTs do not diagnose sleep apnea or prescribe sleep medication.
What physical therapy does
Physical therapy does not replace sleep medicine or mental health care. But it can help you identify how sleep is affecting recovery and build habits that support your plan.
In PT, this may include:
- Sleep screening. Your PT can use questions or brief tools to identify insomnia, poor sleep quality, or possible sleep apnea, then refer when needed.
- Exercise timing. Regular physical activity improves sleep quality. For many people, moderate evening exercise is not a problem, but hard training close to bedtime can leave the body too activated.
- Relaxation and breathing. Progressive muscle relaxation and diaphragmatic breathing can help calm the nervous system. They are not replacements for specialized insomnia care, but they can be part of a safe routine.
- Positioning and symptom management. Back pain, shoulder pain, knee replacement, or surgical recovery may require changes in sleep position, pillows, or strategies for getting in and out of bed without spiking pain.
- Appropriate referral. If you have nightmares, hypervigilance, panic attacks, suspected sleep apnea, or moderate-to-severe insomnia, care should involve a sleep medicine provider, mental health professional, or the VA.
Cognitive behavioral therapy for insomnia (CBT-I) is the first-line treatment for insomnia. Sleep hygiene by itself — turning off screens, avoiding late caffeine, keeping a routine — can help, but it usually does not resolve clinical insomnia, especially when PTSD or chronic pain is involved.
What you can expect
Improving sleep rarely happens overnight. Some people first notice less irritability or better energy. Others notice they tolerate exercise better, pain flares settle faster, or recovery after a session feels easier.
Progress depends on many factors: how long pain has been present, PTSD, TBI, medications, sleep apnea, alcohol use, stress, and routine consistency. If sleep has been disrupted for years, the plan should be gradual. The goal is not perfect sleep. The goal is giving your body more real chances to recover.
When to seek help
Seek professional help if you have:
- Insomnia lasting more than several weeks and affecting daily function
- Loud snoring, breathing pauses, or heavy daytime sleepiness
- Nightmares, hypervigilance, or intrusive memories that keep you from sleeping
- Falls, confusion, or marked drowsiness after taking sleep medication
- New pain, weakness, numbness, or loss of bladder or bowel control
If you are in crisis or thinking about harming yourself, the Veterans Crisis Line is available 24/7 at 988 (press 1) or by text at 838255.
Sources
- Global prevalence of poor sleep quality in military personnel and veterans. Sleep Medicine Reviews, 2023
- Sleep disorders in the Veterans Health Administration. Sleep Medicine Reviews, 2020
- Sleep and pain relationship: review and path forward. The Journal of Pain, 2013
- Bidirectional relationship between sleep problems and chronic musculoskeletal pain. Pain, 2024
- Sleep deprivation and pain sensitivity: meta-analysis. Sleep Medicine Reviews, 2022
- Acute sleep deprivation and muscle protein synthesis. Physiological Reports, 2021
- Sleep and motor memory consolidation: meta-analysis of 48 studies. Neuroscience & Biobehavioral Reviews, 2015
- CBT-I in people with chronic disease: systematic review and meta-analysis. JAMA, 2025
- CBT-I in veterans with PTSD: randomized controlled trial. Sleep, 2014
- Physical activity and sleep: umbrella review. Sleep Medicine Reviews, 2021
- Role of physical therapists in sleep health. APTA House of Delegates Position HOD P06-20-39-09, 2020